Yesterday I’m walking home from school and I look up to see some strange guy in a hard hat at the far end of the block waving at me with his arm. I look around for a minute and see that there’s some kind of construction going on and I realize he wants me to cross to the other side of the street. So I do. But it miffs me a bit, because I dislike it when anyone assumes authority over me that’s not clearly theirs.

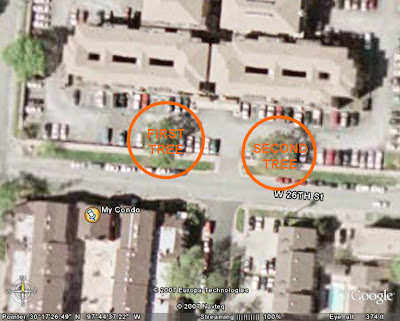
As I get near my condo, at 2529 Rio Grande, I realize what’s going on: They’re knocking down trees, and not little ones either. Just inside the stone wall which is all that remains of the seedy block of furnished apartments that used to occupy the lot immediately north of my building, stood these two proud 40-ft. oak trees, just to either side of the main gate. I don’t know how old they might have been, but I bet they predated the complex that was demolished around them. The workers have to clear the sidewalks because the branches are large and heavy and overhang them to some extent.
Now, I don’t know if it was because I was already a bit grumpy with these guys, or solely because I was offended at the casual destruction of the beautiful old trees in my neighborhood, but I decided I was going to make a hard time for these workers, if possible, and in the best situation maybe stop them from killing the trees. I’m not such a radical (or maybe brave) person as to strap myself to one of the trunks, and it didn’t really look like there would be time to make it to the hardware store and buy chain and a padlock for that purpose before they were finished, anyway.

So I did the only thing I knew to do, which was call the city. I know Austin has fairly tough municipal regulations regarding the felling of trees inside the city limits. I thought maybe I could at least verify that they had a permit to cut down these trees and get them stopped or at least fined if they didn’t. The woman who answered the city information line was confused by my request at first: “There’s a tree you want to cut down?” she said. “No,” I explained, “I’m concerned that I’m witnessing the illegal felling of a protected tree.” There was a pause, and then she said, “Hold on, I’ll have to ask about that one.” So I get the hold muzak, which is an impossibly banal counterpoint to the scene of arboreal slaughter outside my window. While I’m waiting on hold, the destruction of the first tree is completed and the excavator starts filling in the hole left by the torn-out roots.

Eventually the woman returns to the phone, and it’s clear that she now understands and appreciates my situation. “You need to speak to the City Arborist,” she tells me, and gives his name (which I never figured out how to spell, and hence will not include here), and his number, which is 512-974-1876. “I’m sorry it took so long for me to figure that out,” she says. I tell her it’s OK, and she thanks me for calling. It’s obvious at this point that she’s on my side.

I call the Arborist and get his answering machine. The excavator is now rumbling toward the second tree. I leave a rambling message about who and where I am and how they sure are beautiful trees and I just wanna make sure the workers are within their legal rights cutting them down. I am conflicted. A large part of me wants to go down and confront the workers, but I realize that will only make them defensive and will not stop them from doing what they’re doing. I pace back and forth for awhile and figure the only thing to do is take pictures so I can make sure they get punished if it turns out they’re breaking the law. So I snap a frame or two and turn back to the computer to work.

There’s a loud CRACK a minute or two later and I go back to the window and see that the excavator has broken a large limb off the second tree. About then the phone rings, and it’s the arborist, who, to my pleasure, sounds concerned and gets right to the point: “Tell me what you’re seeing,” he says. And I do. As I’m talking, the excavator repositions itself and strikes downward into the tree’s crotch, splitting the trunk, and I realize that there’s no stopping them at this point. I tell the arborist as much. “But I took pictures,” I explain, “in case it turns out that what they’ve done is illegal.”

“Where are you again?” he asks. “West Campus,” I tell him. “Do you know the neighborhood?” He doesn’t. “Do you have an address?” Apparently he’s got a database of some sort that lists permit-holders. I don’t know the exact address, but I can extrapolate from mine and take a guess: “Try 2601.” A minute later he comes back and says, “Yes, there’s a permit to develop that property,” which I understand from his disappointed tone to mean that there’s nothing to be done. Apparently the rule in Austin is that private homeowners need a permit to fell any tree with a diameter of 19 inches or greater, but that developers have more flexibility. The arborist can’t tell me what the specific site plan calls for with respect to these particular trees, but he can tell me that there is a plan and it’s been approved, so in all likelihood these guys are acting in accordance with it and hence within the bounds of law. I thank him and he thanks me, and before we hang up he asks me to call again any time I’m suspicious of tree-related crime, because his office depends almost completely on concerned citizens/nosy neighbors like me to catch and prevent the illegal destruction of trees. I assure him that I will.
And that’s where the story peters out. I wanted to do something but I didn’t, basically, and although I got some sympathetic voices on the phone none of it changes the basic fact of the matter, which is that there are now two muddy holes in the ground where there were once two live, beautiful, healthy trees. And I stood to one side and watched as a man with a machine tore them up. Should I have tried, physically, to intervene? Should I have obeyed that impulse to chain myself to the trunk? I don’t know the spirit of a tree, but I know how hard it was to watch them be destroyed. It was like a crime was happening out on the street, in broad daylight, and everyone was just walking by indifferently. I didn’t want to be the apathetic one; I wanted to be the one who gave a shit. But I tried to be a civilized adult about the whole thing and now I regret it. Even if I hadn’t, ultimately, saved those particular trees, a show of strength might’ve brought some attention to the subject, might’ve made the developers or the city authorities or whoever think twice the next time they decided to hire out that kind of a dirty job. But in the end I was just like everyone else: Too busy with my own concerns to take hours out of my day to worry about something as simple as the killing of a tree.



{kind=link}